





The Cholesterol Code: a scientific review of the documentary








The Cholesterol Code is a 2026 documentary film (directed by Jennifer Isenhart, built around citizen scientist Dave Feldman) arguing that high LDL cholesterol is harmless for lean, metabolically healthy people on ketogenic diets. In this scientific review, nutritionist TJ Waterfall and Dr Matthew Nagra weigh the film's claims against the evidence: it is right that metabolic health matters, but its central claim — that very high LDL is benign — runs against decades of genetics, epidemiology and randomised trials showing ApoB-containing lipoproteins cause heart disease.



What is The Cholesterol Code about?
The Cholesterol Code presents a compelling challenge to mainstream thinking on cholesterol, particularly in the context of ketogenic diets. The central argument is that high LDL cholesterol – especially in lean, metabolically healthy individuals following low-carbohydrate diets – may not be inherently harmful, and that modern medicine has overemphasised cholesterol while underappreciating other cardiometabolic risk factors such as insulin resistance.
The film presents these ideas with confidence and emotional appeal, often framing them as a courageous challenge to an outdated medical consensus. But when examined through a scientific lens, it becomes obvious that many of the arguments rely heavily on anecdotes, selective interpretation of data, and overconfidence in early-stage hypotheses. At the same time, the film downplays the scale, consistency, and convergence of evidence supporting LDL cholesterol and apoB-containing lipoproteins as causal drivers of atherosclerotic cardiovascular disease.
What the film gets right
Before getting into the major scientific issues with the film, it’s important to acknowledge that not everything it says is wrong. In fact, there are several areas where the documentary broadly aligns with current evidence.
1. Metabolic health clearly matters. Insulin resistance, type 2 diabetes, hypertension, smoking, obesity, physical inactivity, and chronic inflammation are all important contributors to cardiovascular risk. Improving these factors can meaningfully reduce disease risk and improve overall health outcomes.
2. Some individuals experience genuine short-term benefits from carbohydrate-restricted diets. Some report improvements in body weight, appetite regulation, glycaemic control, triglycerides, and certain clinical conditions such as epilepsy when following low-carbohydrate or ketogenic diets. These experiences should not be dismissed, and people dealing with complex health issues deserve nuanced, compassionate, evidence-based care.
Where the film misses the mark
Although the film does get some aspects right, many of its broader conclusions rely on weak inferences, selective use of evidence, and major logical leaps that simply don’t stack up. Collectively, these arguments leave viewers with the impression that high LDL cholesterol is largely harmless in metabolically healthy individuals, a conclusion that goes far beyond what the current evidence can reliably support.
Let’s break down some of the key fallacies, claims and assumptions made in the film that are not well supported:
The role of anecdote in science
Much of the film’s persuasive power comes from personal stories. These include individuals with conditions such as type 1 diabetes, bipolar disorder, inflammatory bowel disease, and eating disorders who report improvements on ketogenic diets. Others come from otherwise healthy individuals who feel great despite having high LDL cholesterol levels. On the surface, these stories may sound compelling and are emotionally powerful, but they’re not evidence of causality. That’s because anecdotes are:
• Uncontrolled: They lack a comparison group or control conditions, so you can’t isolate what actually caused the outcome.
• Highly selective: They tend to highlight unusual or successful cases while overlooking the many instances where the same approach didn’t work.
• Extremely vulnerable to bias: They are influenced by factors like placebo effects, recall bias, and personal expectations, making them unreliable indicators of cause and effect.
You can generate or find anecdotes to support literally any position… Dig hard enough and you’ll be able to find a centenarian who smokes every day and feels great. That doesn’t mean that habit should be adopted by everyone, or even that it was the best path for that individual.
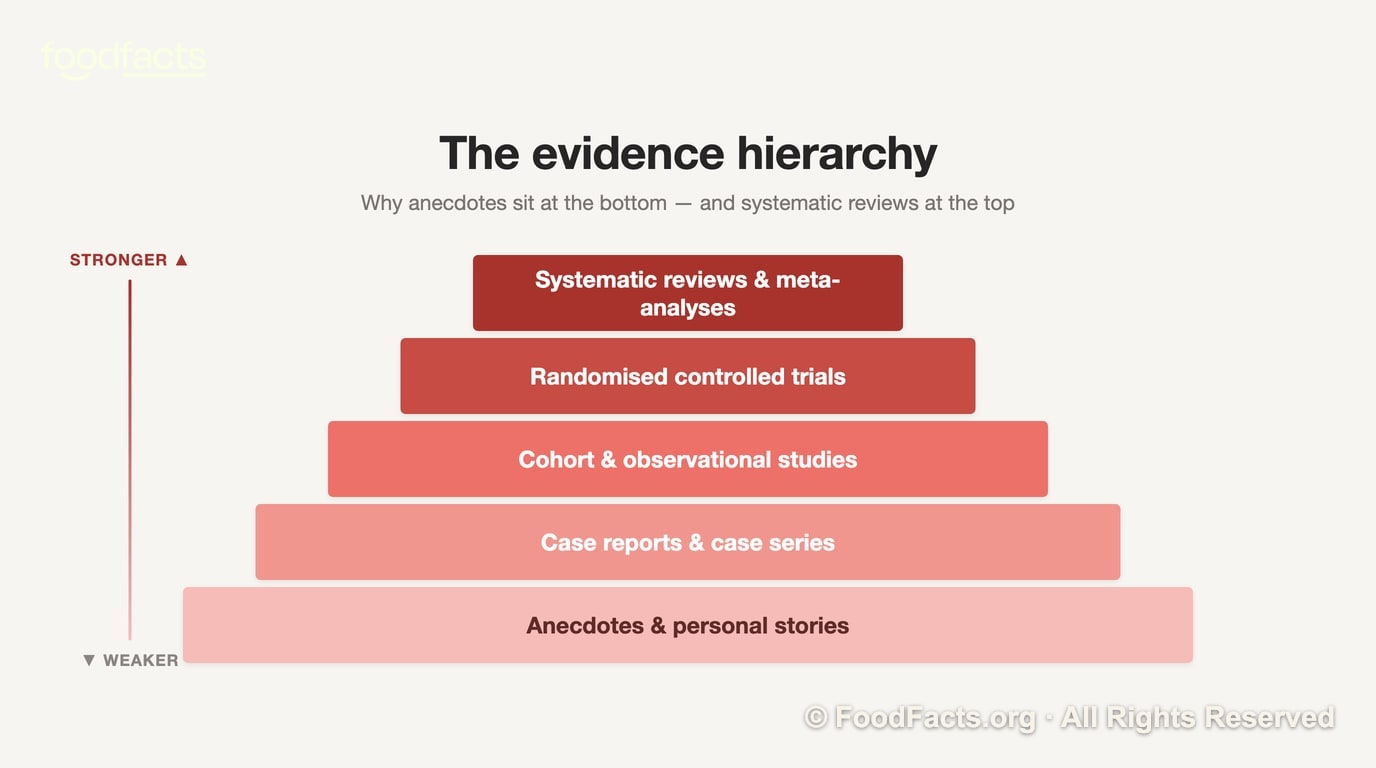
Anecdotes can be useful, however, for generating hypotheses. They can also be used to illustrate findings that align with existing evidence, which can be seen as bringing data “to life” (e.g. a heavy smoker regaining lung function after quitting could be motivational for others, beyond just showing them the data or statistics). But when anecdotes are used to challenge well-established causal relationships, they should be interpreted with extreme caution.
“Cholesterol is essential, so it can’t be harmful”
The film emphasises how cholesterol is essential for human life, and the important roles it plays in cell membranes, hormone production, bile acids, and vitamin D synthesis. All of this is true, but is irrelevant to the question being asked, which is whether there is increased risk at high levels.
Many compounds that are essential to life can be harmful in excess. Sodium is essential, but we know that consuming too much causes high blood pressure; glucose is essential (the body produces it from proteins and fat if intake is too low) but chronically elevated levels are central to diabetes and its complications.
So the existence of a physiological role does not imply safety at high levels. The issue is not whether cholesterol is necessary – it is whether elevated circulating LDL cholesterol contributes to atherosclerosis. And the evidence consistently shows that it does.
“LDL evidence comes from unhealthy populations”
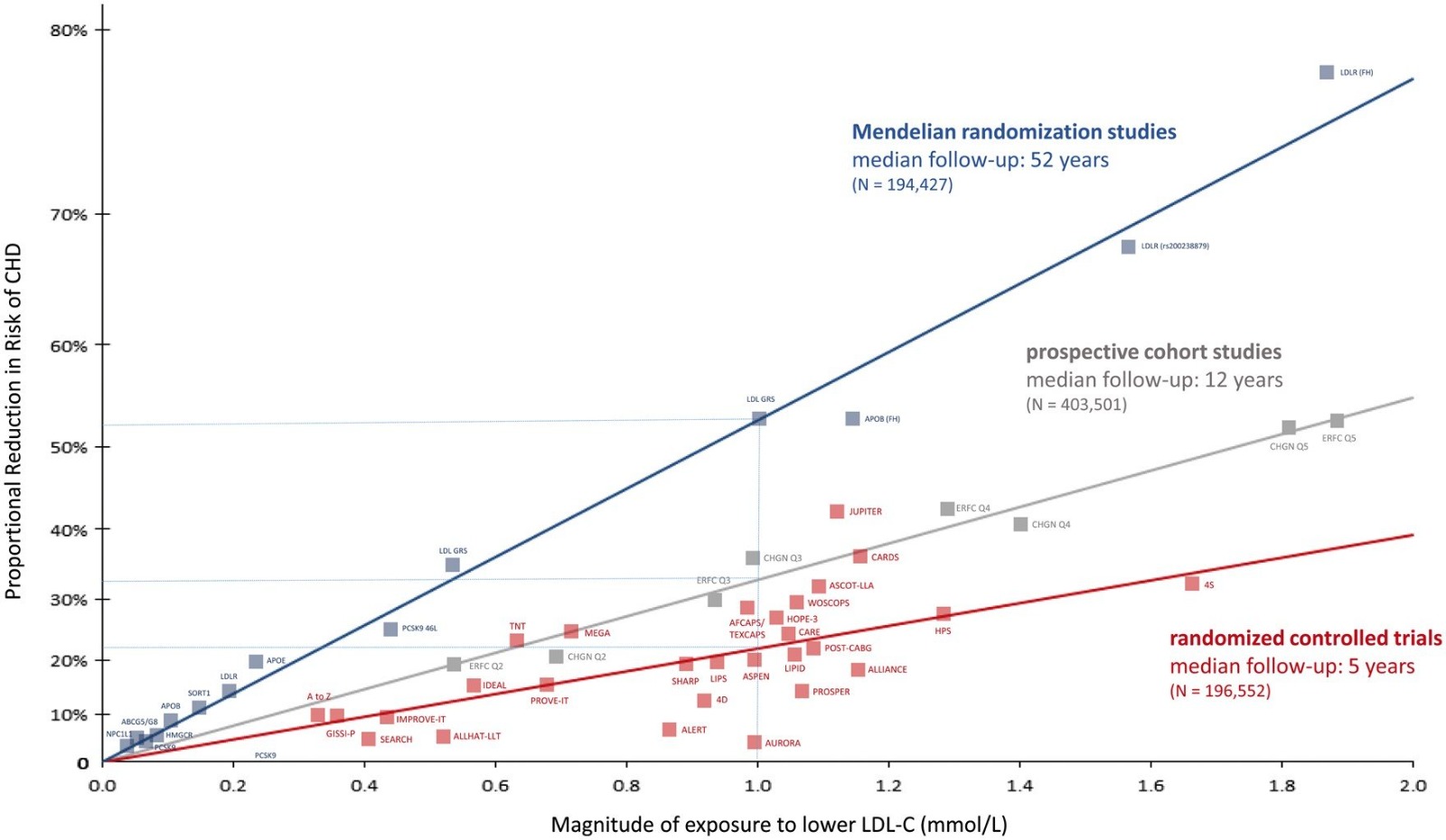
This is a common argument, but it simply doesn’t hold when looking at the full body of evidence. The causal role of LDL cholesterol in atherosclerosis is supported by multiple independent lines of evidence:
1. Observational data: Meta-analyses of prospective cohort studies that adjust for lifestyle factors and metabolic health consistently find that LDL cholesterol is associated with atherosclerosis (1,2).
This is true even when studied specifically in adults without any other cardiovascular risk factors such as smoking, family history, obesity, hypertension, diabetes, or dyslipidemia (3).
2. Mendelian randomisation studies: Some people inherit genetic variants that raise LDL cholesterol. Because these genes are randomly assigned, Mendelian randomisation studies can assess whether lifelong exposure to higher LDL increases heart disease risk, largely independent of lifestyle factors or other risk factors.
A recent meta-analysis of over 20 such studies, involving nearly 6 million participants, found a significant causal association between LDL cholesterol, ApoB, and coronary artery disease (4).
3. Randomised controlled trials: Meta-analyses of randomised controlled trials also show that lowering LDL cholesterol – whether through use of statins or non-statin therapies, including diet – significantly lowers cardiovascular events like heart attacks (5,6). Importantly, these findings are consistent across populations and contexts.
Creating a false dichotomy
The film often frames insulin resistance and LDL as competing explanations for cardiovascular disease. But in reality, they are not mutually exclusive: both matter.
Improving metabolic health is important – but this does not negate the causal role of LDL cholesterol. Even in individuals who are otherwise metabolically healthy, elevated LDL cholesterol remains associated with increased risk.
A recent review published in the Journal of the American Heart Association concluded that the proposed theory that keto-driven LDL elevations may be benign in otherwise metabolically healthy individuals lacks any credible evidence (7).

And while ketogenic diets may improve insulin sensitivity in adults with type-2 diabetes, evidence shows those improvements are simply attributable to the weight loss it promotes. In a recent study where overweight obese adults with type-2 diabetes were subject to a low carbohydrate ketogenic diet that was specifically designed to maintain body weight, there were no beneficial effects on glucose tolerance, insulin sensitivity, or other metabolic parameters (8).
“High HDL and low triglycerides offset LDL”
High HDL cholesterol was historically thought to be protective against atherosclerotic cardiovascular disease, because high blood levels were associated with decreased risk in observational data.
But – unlike the evidence for LDL cholesterol – the link was found to be only correlational, not causal. Later Mendelian randomisation found genetic variants that raise HDL did not reduce heart disease risk, and randomised controlled trials found that pharmacologically raising HDL did not consistently reduce cardiovascular mortality or events (9,10).
On the other hand, lowering triglycerides can be protective, but still doesn’t neutralise the risk of high LDL cholesterol. This argument relies heavily on small, short-term datasets, including the Keto-CTA study, which we examine in more detail below and has glaring limitations.
There are also well-established ways to improve triglycerides and HDL – such as weight loss, improved diet quality, and physical activity – that can benefit other aspects of health and don’t simultaneously increase LDL cholesterol (11-13).
The implication of conspiracy
A recurring theme throughout the film is the suggestion that mainstream medicine has fundamentally misunderstood cholesterol, and that the focus on LDL cholesterol is largely driven by pharmaceutical interests rather than good science. The narrative creates a strong “us vs them” dynamic: conventional medicine is portrayed as dogmatic, financially compromised, and unwilling to challenge its own assumptions, while the filmmakers position themselves as independent truth-seekers exposing what others refuse to acknowledge.
But this framing becomes harder to sustain when the study at the center of the film is examined more closely: the study’s primary funder, the Citizen Science Foundation, was founded and led by Dave Feldman – the originator and leading advocate of the Lean Mass Hyper-Responder (LMHR) hypothesis itself.
Feldman was not a detached observer testing a neutral scientific question; he had spent years publicly promoting the idea before the study began. His involvement in funding, recruitment, interpretation, and public communication, combined with the use of a highly self-selected participant pool drawn largely from communities already aligned with the hypothesis, creates a level of researcher-participant alignment that warrants cautious interpretation of the findings.
If the film is encouraging viewers to be skeptical of potential bias and conflicts of interest in mainstream science, then the same level of scrutiny should also be applied here.
The broader “Big Pharma invented the LDL hypothesis” implication is also difficult to reconcile with the actual history of lipid research. For decades, pharmaceutical companies had enormous financial incentive for HDL cholesterol to be causally protective against cardiovascular disease, based on initial observational research.
But, as described above, when the hypothesis was properly tested, the evidence failed to support it. Despite the enormous commercial potential, the HDL hypothesis was largely abandoned because the outcomes did not support a causal effect (meanwhile, science consistently demonstrates the causal relationship between LDL cholesterol and cardiovascular disease).
CAC and CTA scans as reassurance
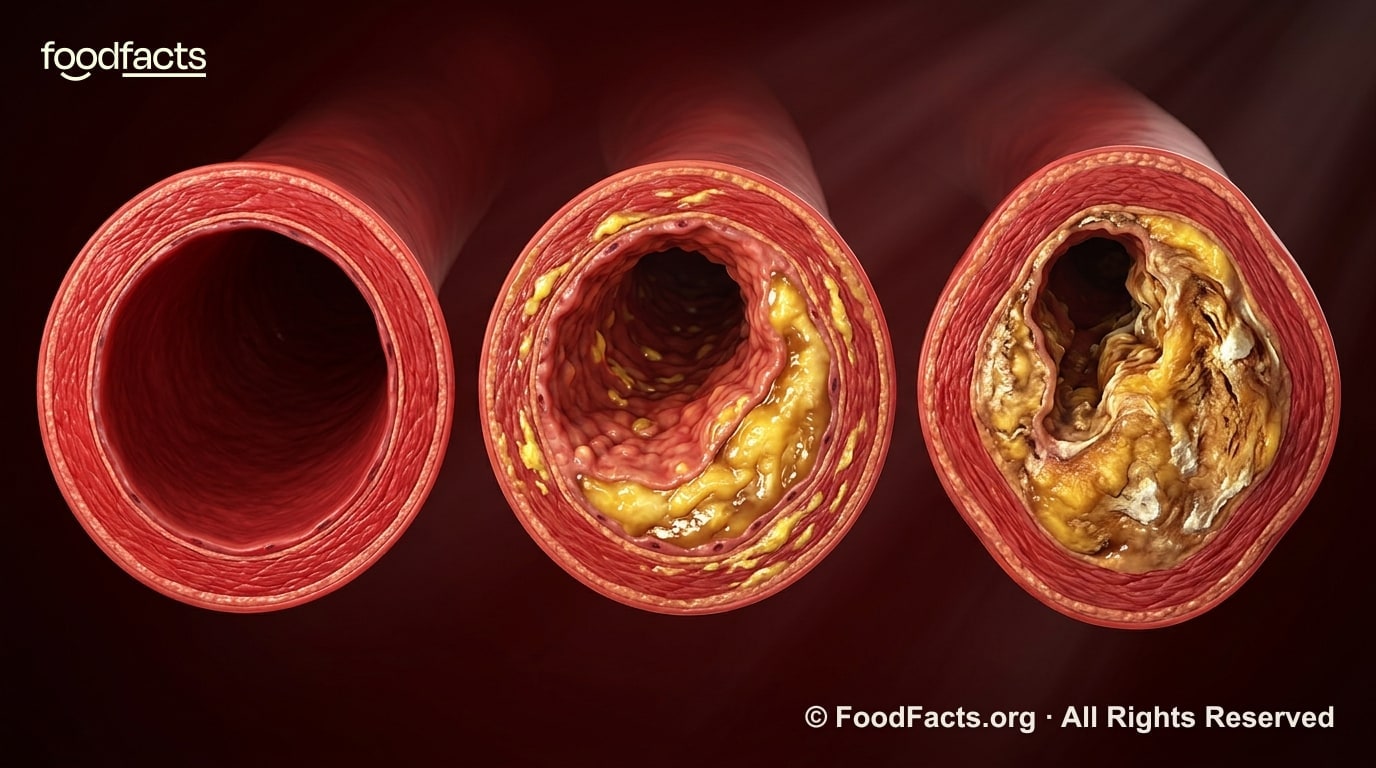
Coronary artery calcium (CAC) and CT angiography (CTA) scans are useful tools, but they have important limitations that the film tends to gloss over.
The film highlights individuals with extremely high LDL cholesterol who have CAC scores of zero and suggests this demonstrates an absence of coronary disease. But a CAC score of zero does not mean zero atherosclerosis. CAC scans only detect calcified plaque, which typically develops later in the disease process (14). Non-calcified ("soft") plaque can still be present, even when CAC is zero. In fact, studies have found that around 10% of asymptomatic people with a CAC score of zero have detectable non-calcified plaque, and elevated LDL cholesterol predicts its presence (15,16).
This is particularly relevant in younger individuals. Atherosclerosis develops over decades, and calcification often appears much later than the initial plaque formation (17). Someone may therefore have a CAC score of zero despite prolonged exposure to elevated LDL cholesterol.

The film also presents CTA findings as reassuring evidence that high LDL may be harmless. While CTA can provide valuable information about non-calcified plaque, these measurements also have limitations. For instance, there is currently a lack of certainty on how to define plaque progression and what is considered a significant change (18). The Keto-CTA study relied on specialised AI software to detect and quantify very small plaque changes that may not be visible to clinicians. However, experts have noted that the clinical significance of these measurements remains uncertain, and there is currently no clear consensus on what constitutes meaningful progression versus normal measurement variability (19).
Importantly, atherosclerosis is a slow-moving disease. Current guidance generally recommends years between repeat scans when assessing progression, whereas the Keto-CTA study followed participants for only one year. Small apparent increases or decreases in plaque volume over such a short period may simply reflect measurement noise rather than true biological change. Absence of evidence is not evidence of absence.
Ultimately, CAC and CTA scans can help estimate current risk, but they cannot reliably determine whether decades of exposure to elevated ApoB-containing lipoproteins will be safe in the long term (20). Atherosclerosis is dynamic, and risk is determined by cumulative exposure over time, not short-term fluctuations.
Over-reliance on the Keto-CTA study
The film places significant weight on the “Keto-CTA” study as evidence that high LDL cholesterol may be harmless in lean, metabolically healthy people following ketogenic diets. But this interpretation is not justified.
Firstly, the study was small, followed participants for just one year, and included a relatively young, healthy group with low cardiovascular risk. Atherosclerosis develops over decades, not months, making it difficult to draw meaningful conclusions about long-term risk from such a short study.
Secondly, the study did not include a comparison group with lower LDL cholesterol levels. Instead, it effectively assessed whether, among people who already have very high LDL cholesterol, slightly higher levels predict short-term changes in plaque burden over a one-year period. These are fundamentally different questions.
The study also began after participants had already spent years following low-carbohydrate diets with elevated LDL cholesterol. This means any plaque development that occurred before the study started was not captured. The participants were also recruited from online communities centred around carbohydrate restricted diets, which introduces significant potential for selection and survivorship bias, because individuals who discontinued these diets or experienced adverse outcomes would be less likely to be represented.
Importantly, the film also gives the impression that plaque progression observed during the study was minimal, even though median non-calcified plaque volume increased by approximately 37% over the one-year follow-up period, with 85% of participants showing progression and a sizeable proportion of participants meeting the study's own criteria for significant plaque progression (21). The study was neither designed nor powered to conclude that ApoB doesn’t predict risk, just because a minority of participants showed no progression or regression, and the findings certainly don’t outweigh the substantial broader evidence linking long-term exposure to elevated LDL cholesterol and ApoB with cardiovascular disease.
It's also worth noting that the study had not yet undergone peer review at the time the film was released, which is an important part of the scientific process. It is therefore highly unusual to place so much emphasis on a single, unpublished study while simultaneously dismissing decades of rigorous evidence that consistently points in the other direction.
Ultimately, the Keto-CTA study is an interesting early piece of research, but it does not overturn the large body of evidence from genetics, epidemiology, and clinical trials showing that ApoB-containing lipoproteins play a causal role in atherosclerosis.
Carbohydrate reintroduction experiments
The film presents examples where adding carbohydrates rapidly lowers LDL in certain individuals. This simply demonstrates that, under certain metabolic conditions, LDL particles are being used more heavily for energy and fuel transport when carbohydrate availability is very low. In other words, the rise in LDL may partly reflect an adaptation to altered fuel use.
But explaining why LDL rises doesn’t in any way prove that the rise is harmless. Mechanism and clinical outcome are two separate questions.
We understand many biological mechanisms that can transiently alter biomarkers, but the key question is whether long-term exposure increases disease risk. In the case of LDL cholesterol, multiple lines of evidence, including genetics, prospective epidemiology, and randomized trials, converge on the conclusion that higher cumulative exposure increases atherosclerotic cardiovascular disease risk.
So even if a ketogenic or very low-carbohydrate diet causes LDL to rise for a mechanistically understandable reason, that does not automatically exempt those particles from contributing to atherosclerosis. The body may have a reason for elevating LDL under those conditions, but that reason does not establish safety.
Generalising from specific clinical anecdotes
One of the film’s recurring tactics is to highlight specific clinical applications of ketogenic diets and then imply that these benefits can be generalized to the broader population. But this is a major logical leap.
Take epilepsy, for example. The use of ketogenic diets for epilepsy is not a newly discovered or suppressed concept, despite the way the film sometimes frames it. In fact, ketogenic diets were originally developed in the 1920s after physicians observed that fasting could reduce seizures in some patients with epilepsy. Because long-term fasting is not sustainable, researchers developed dietary protocols designed to mimic some of the metabolic effects of fasting while still allowing patients to eat.

Importantly, these therapeutic ketogenic diets differ substantially from the popularized “keto” diets promoted online today. Classical medical ketogenic diets are extremely high in fat, tightly controlled, and often relatively low in protein, in some cases providing as little as 8% of calories from protein (22). They’re also typically implemented in specific clinical settings, often for drug-resistant epilepsy and under close medical supervision.
Even in epilepsy care, ketogenic diets are not considered universally appropriate or risk-free. Their use is evaluated on a case-by-case basis, weighing potential benefits against nutritional adequacy, side effects, long-term adherence, quality of life, and individual patient circumstances.
Even where therapeutic benefits exist, that does not automatically eliminate potential cardiovascular concerns associated with persistently elevated LDL levels. A diet may improve one condition while increasing risk in another, which is why nutrition interventions should be evaluated holistically rather than through a single outcome in isolation.
Ultimately, therapeutic ketogenic diets should be viewed as targeted clinical tools for very specific contexts – not blanket evidence that very low-carbohydrate diets are inherently optimal or risk-free for the general population.
Omitting potential risks
There are other important considerations largely absent from the film that could be considered misleading – or even outright irresponsible – to leave out.
Firstly, the type of fat consumed matters. Replacing saturated fats with unsaturated fats – particularly polyunsaturated fats – has consistently been shown to reduce LDL cholesterol and cardiovascular risk in both controlled feeding studies and long-term clinical research (23,24). Research even suggests that ketogenic diets emphasising polyunsaturated fats may induce ketosis more effectively, improve insulin sensitivity, and avoid the marked increases in total and LDL cholesterol often observed with saturated fat–dominant ketogenic diets (25). Framing the discussion primarily around carbohydrate restriction, without adequately addressing fat quality, overlooks a major component of cardiovascular nutrition science.

The film also brushes over the concept of cumulative exposure. Atherosclerosis develops over decades, and evidence from genetics, epidemiology, and randomized trials suggests that both the magnitude and duration of exposure to LDL cholesterol influence risk. In other words, even if someone is metabolically healthy in the short term, prolonged exposure to elevated LDL can contribute to plaque development over time.
Another underrepresented issue is nutrient adequacy. Recent reviews assessing carbohydrate-restricted and ketogenic diets report an increased risk of inadequate intake of several micronutrients and beneficial dietary compounds, primarily because important food groups such as legumes, whole grains, fruits, and starchy vegetables are often substantially restricted (26,27). A key example is fibre, intake of which is consistently associated with improved cardiometabolic health, healthier blood lipid profiles, improved glycaemic control, and lower risk of cardiovascular disease and colorectal cancer. Fibre also plays an important role in supporting gut microbiome health and short-chain fatty acid production, which influences whole-body health (28,29).
None of this means ketogenic diets cannot have therapeutic applications or help certain individuals. But these broader considerations are essential for interpreting the totality of evidence around long-term health and cardiovascular risk.
The verdict: is The Cholesterol Code accurate?
The observation that some lean, physically active individuals experience dramatic increases in LDL-C and ApoB on carbohydrate-restricted diets while maintaining favourable markers elsewhere deserves careful study. But an interesting hypothesis is not the same as overturning decades of evidence.
The film is right about some things. Metabolic health matters. Ketogenic diets may help certain individuals in specific contexts, particularly for glycaemic control or appetite regulation in the short term.
However, the documentary repeatedly implies that very high LDL-C or ApoB may be benign, or even advantageous, in metabolically healthy individuals. That conclusion goes far beyond what the evidence currently supports.
The causal role of ApoB-containing lipoproteins in atherosclerotic cardiovascular disease is supported by an enormous body of evidence spanning genetics, epidemiology, Mendelian randomization studies, mechanistic research, and randomized LDL-lowering trials. To dismiss this evidence largely on the basis of short-term observations, surrogate markers, and highly selective anecdotes is scientifically difficult to justify.
Atherosclerosis develops cumulatively over decades, not months. Improvements in some metabolic markers do not somehow render chronically elevated ApoB harmless. And while the film spends considerable time challenging the conventional understanding of cardiovascular risk, it offers little long-term outcome data capable of supporting such extraordinary claims.
Ultimately, the burden of proof lies with those arguing that markedly elevated ApoB is safe despite decades of evidence suggesting otherwise. Until robust long-term evidence demonstrates that these elevations do not increase cardiovascular risk, elevated ApoB should be treated as what the overwhelming body of evidence indicates it to be: a causal driver of atherosclerotic cardiovascular disease.
Frequently asked questions
Is The Cholesterol Code accurate?
Partly. The film is right that metabolic health matters and that ketogenic diets can help some people in the short term. But its central claim — that very high LDL cholesterol is harmless in lean, metabolically healthy people — is not supported by the evidence. Decades of genetics, prospective epidemiology and randomised trials show that ApoB-containing lipoproteins, including LDL, are a causal driver of atherosclerotic cardiovascular disease.
What is The Cholesterol Code film about?
The Cholesterol Code is a 2026 documentary, directed by Jennifer Isenhart and built around citizen scientist Dave Feldman, that questions the mainstream view of LDL cholesterol. It argues that high LDL may be benign for lean, metabolically healthy people on low-carbohydrate or ketogenic diets — the "Lean Mass Hyper-Responder" hypothesis.
Is high LDL cholesterol on a keto diet dangerous?
On current evidence, persistently elevated LDL and ApoB raise cardiovascular risk regardless of how they are produced — including when a ketogenic diet drives them up. A mechanistic explanation for why LDL rises does not make those particles harmless. Anyone whose LDL rises substantially on a low-carb diet should discuss it with a qualified clinician.
What is the Keto-CTA study, and does it prove high LDL is safe?
The Keto-CTA study followed lean "hyper-responders" with very high LDL for one year using CT angiography. It was small, uncontrolled, short, and recruited from low-carb communities — and median non-calcified plaque actually rose by roughly 37%, with most participants showing progression. It is an interesting early dataset, not evidence that high LDL is safe, and it had not been peer-reviewed when the film was released.
Who reviewed The Cholesterol Code for FoodFacts?
This scientific review was written by registered nutritionist TJ Waterfall and Dr Matthew Nagra, drawing on 29 peer-reviewed sources listed in the Resources section.

Stand Against Nutrition Misinformation
Misinformation is a growing threat to our health and planet. At foodfacts.org, we're dedicated to exposing the truth behind misleading food narratives. But we can't do it without your support.
1. Jung, E., Kong, S. Y., Ro, Y. S., Ryu, H. H., & Shin, S. D. (2022). Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies. International journal of environmental research and public health, 19(14), 8272. — PubMed ↗
2. Emerging Risk Factors Collaboration, Di Angelantonio, E., Gao, P., Pennells, L., Kaptoge, S., Caslake, M., Thompson, A., Butterworth, A. S., Sarwar, N., Wormser, D., Saleheen, D., Ballantyne, C. M., Psaty, B. M., Sundström, J., Ridker, P. M., Nagel, D., Gillum, R. F., Ford, I., Ducimetiere, P., Kiechl, S., … Danesh, J. (2012). Lipid-related markers and cardiovascular disease prediction. JAMA, 307(23), 2499–2506. — PubMed ↗
3. Fernández-Friera, L., Fuster, V., López-Melgar, B., Oliva, B., García-Ruiz, J. M., Mendiguren, J., Bueno, H., Pocock, S., Ibáñez, B., Fernández-Ortiz, A., & Sanz, J. (2017). Normal LDL-Cholesterol Levels Are Associated With Subclinical Atherosclerosis in the Absence of Risk Factors. Journal of the American College of Cardiology, 70(24), 2979–2991. — PubMed ↗
4. Yang, R., Wu, S., Zhao, Z., Deng, X., Deng, Q., Wang, D., & Liu, Q. (2026). Causal association between lipoproteins and risk of coronary artery disease-a systematic review and meta-analysis of Mendelian randomization studies. Clinical research in cardiology : official journal of the German Cardiac Society, 115(2), 175–184. — PubMed ↗
5. Kalra, D. K., Ray, K. K., Bajaj, A., Kushner, P. R., Wilcox, M. L., Dicklin, M. R., Kirkpatrick, C. F., & Maki, K. C. (2026). Low-density lipoprotein cholesterol lowering and risk of major adverse cardiovascular events in primary prevention trials: A meta-analysis. Journal of Clinical Lipidology, 20(4), 738–749. — PubMed ↗
6. Silverman, M. G., Ference, B. A., Im, K., Wiviott, S. D., Giugliano, R. P., Grundy, S. M., Braunwald, E., & Sabatine, M. S. (2016). Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA, 316(12), 1289–1297. — PubMed ↗
7. DiMattia, Z. S., & Petersen, K. S. (2026). Ketogenic Diets and Low-Density Lipoprotein Cholesterol in Adults With Normal Weight: An Emerging Clinical Challenge. Journal of the American Heart Association, 15(9), e048903. — PubMed ↗
8. Merovci, A., Finley, B., Hansis-Diarte, A., Neppala, S., Abdul-Ghani, M. A., Cersosimo, E., Triplitt, C., & DeFronzo, R. A. (2024). Effect of weight-maintaining ketogenic diet on glycemic control and insulin sensitivity in obese T2D subjects. BMJ open diabetes research & care, 12(5), e004199. — PubMed ↗
9. Voight, B. F., Peloso, G. M., Orho-Melander, M., Frikke-Schmidt, R., Barbalic, M., Jensen, M. K., Hindy, G., Hólm, H., Ding, E. L., Johnson, T., Schunkert, H., Samani, N. J., Clarke, R., Hopewell, J. C., Thompson, J. F., Li, M., Thorleifsson, G., Newton-Cheh, C., Musunuru, K., Pirruccello, J. P., … Kathiresan, S. (2012). Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet (London, England), 380(9841), 572–580. — PubMed ↗
10. Keene, D., Price, C., Shun-Shin, M. J., & Francis, D. P. (2014). Effect on cardiovascular risk of high density lipoprotein targeted drug treatments niacin, fibrates, and CETP inhibitors: meta-analysis of randomised controlled trials including 117,411 patients. BMJ (Clinical research ed.), 349, g4379. — PubMed ↗
11. Weinstein, S., Maor, E., Kaplan, A., Hod, T., Leibowitz, A., Grossman, E., & Shlomai, G. (2024). Non-Interventional Weight Changes Are Associated with Alterations in Lipid Profiles and in the Triglyceride-to-HDL Cholesterol Ratio. Nutrients, 16(4), 486. — PubMed ↗
12. Faraji, H., Jamshidi, S., Ferrie, S., & Azar, P. S. (2024). The Relationship between Healthy Eating Index and Lipid Profile in Healthy Individuals: A Systematic Review. International journal of preventive medicine, 15, 6. — PubMed ↗
13. Smart, N. A., Downes, D., van der Touw, T., Hada, S., Dieberg, G., Pearson, M. J., Wolden, M., King, N., & Goodman, S. P. J. (2025). The Effect of Exercise Training on Blood Lipids: A Systematic Review and Meta-analysis. Sports medicine (Auckland, N.Z.), 55(1), 67–78. — PubMed ↗
14. Aldana-Bitar, J., Krishnan, S., Ichikawa, K., Kinninger, A., Hubbard, L., Sallam, T., Roy, S., Lakshmanan, S., Budoff, M. J., & Karlsberg, R. P. (2026). NATURal history of coronary PlaquE on cardiac computed tomography in individuals without MACE or lipid-lowering therapy: NATURE-CT study. Journal of cardiovascular computed tomography, S1934-5925(26)00097-3. Advance online publication. — PubMed ↗
15. Sama, C., Abdelhaleem, A., Velu, D., Ditah Chobufo, M., Fongwen, N. T., Budoff, M. J., Roberts, M., Balla, S., Mills, J. D., Njim, T. N., Greathouse, M., Zeb, I., & Hamirani, Y. S. (2024). Non-calcified plaque in asymptomatic patients with zero coronary artery calcium score: A systematic review and meta-analysis. Journal of cardiovascular computed tomography, 18(1), 43–49. — PubMed ↗
16. Andersen, M. H., Jensen, J. M., Kanstrup, H., Sand, N. P. R., Busk, M., Hansen, M. K., Thrane, P. G., Olesen, K. K. W., Nordestgaard, B. G., Blaha, M. J., Maeng, M., Nørgaard, B. L., & Mortensen, M. B. (2025). Low-density lipoprotein cholesterol and cardiovascular risk in the absence of calcifications on computed tomography: the Western Denmark Heart Registry. European heart journal, 46(46), 5062–5072. — PubMed ↗
17. Dzaye, O., Dardari, Z. A., Cainzos-Achirica, M., Blankstein, R., Szklo, M., Budoff, M. J., Lima, J. A. C., Blumenthal, R. S., Nasir, K., & Blaha, M. J. (2020). Incidence of New Coronary Calcification: Time to Conversion From CAC = 0. Journal of the American College of Cardiology, 75(13), 1610–1613. — PubMed ↗
18. Bienstock, S., Lin, F., Blankstein, R., Leipsic, J., Cardoso, R., Ahmadi, A., Gelijns, A., Patel, K., Baldassarre, L. A., Hadley, M., LaRocca, G., Sanz, J., Narula, J., Chandrashekhar, Y. S., Shaw, L. J., & Fuster, V. (2023). Advances in Coronary Computed Tomographic Angiographic Imaging of Atherosclerosis for Risk Stratification and Preventive Care. JACC. Cardiovascular imaging, 16(8), 1099–1115. — PubMed ↗
19. Chandrashekhar, Y., Blankstein, R., Shaw, L. J., Ferencik, M., Leipsic, J., Trinquart, L., Villines, T. C., & ACC Quantitative Coronary Plaque Analysis Symposium Collaborators (2026). Quantitative Coronary Plaque Analysis in Clinical Practice: 2025 ACC Scientific Statement: A Report of the American College of Cardiology. JACC. Cardiovascular imaging, 19(5), 637–652. — PubMed ↗
20. DiMattia, Z. S., & Petersen, K. S. (2026). Ketogenic Diets and Low-Density Lipoprotein Cholesterol in Adults With Normal Weight: An Emerging Clinical Challenge. Journal of the American Heart Association, 15(9), e048903. — PubMed ↗
21. Budoff, M. J., Kinninger, A., Manubolu, V. S., Norwitz, N. G., Feldman, D. A., & Soto-Mota, A. (2026). The impact of sustained LDL-C elevation on plaque changes: Primary coronary plaque progression results from the Keto CTA Study [Preprint]. medRxiv. — medRxiv preprint ↗
22. McDonald TJW, Cervenka MC. Ketogenic Diets for Adults With Highly Refractory Epilepsy. Epilepsy Curr. 2017 Nov-Dec;17(6):346-350. doi: 10.5698/1535-7597.17.6.346. PMID: 29217974; PMCID: PMC5706352. — PubMed ↗
23. Sacks, F. M., Lichtenstein, A. H., Wu, J. H. Y., Appel, L. J., Creager, M. A., Kris-Etherton, P. M., Miller, M., Rimm, E. B., Rudel, L. L., Robinson, J. G., Stone, N. J., Van Horn, L. V., & American Heart Association (2017). Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation, 136(3), e1–e23. — PubMed ↗
24. Hooper, L., Martin, N., Jimoh, O. F., Kirk, C., Foster, E., & Abdelhamid, A. S. (2020). Reduction in saturated fat intake for cardiovascular disease. The Cochrane database of systematic reviews, 5(5), CD011737. — PubMed ↗
25. Fuehrlein, B. S., Rutenberg, M. S., Silver, J. N., Warren, M. W., Theriaque, D. W., Duncan, G. E., Stacpoole, P. W., & Brantly, M. L. (2004). Differential metabolic effects of saturated versus polyunsaturated fats in ketogenic diets. The Journal of clinical endocrinology and metabolism, 89(4), 1641–1645. — PubMed ↗
26. Churuangsuk, C., Griffiths, D., Lean, M. E. J., & Combet, E. (2019). Impacts of carbohydrate-restricted diets on micronutrient intakes and status: A systematic review. Obesity reviews : an official journal of the International Association for the Study of Obesity, 20(8), 1132–1147. — PubMed ↗
27. Crosby, L., Davis, B., Joshi, S., Jardine, M., Paul, J., Neola, M., & Barnard, N. D. (2021). Ketogenic Diets and Chronic Disease: Weighing the Benefits Against the Risks. Frontiers in nutrition, 8, 702802. — PubMed ↗
28. Reynolds, A., Mann, J., Cummings, J., Winter, N., Mete, E., & Te Morenga, L. (2019). Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet (London, England), 393(10170), 434–445. — PubMed ↗
29. Makki, K., Deehan, E. C., Walter, J., & Bäckhed, F. (2018). The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell host & microbe, 23(6), 705–715. — PubMed ↗




foodfacts.org is an independent non-profit fact-checking platform dedicated to exposing misinformation in the food industry. We provide transparent, science-based insights on nutrition, health, and environmental impacts, empowering consumers to make informed choices for a healthier society and planet.








.svg)
