





Did the New US dietary guidelines clear saturated fat? The claim fact-checked








In a recent post about “a deep dive on saturated fat,” Dr Mark Hyman argues that the new U.S. Dietary Guidelines show we have previously been misled about saturated fat. He further claims that saturated fat from grass‑fed beef, eggs, and dairy is different from saturated fat in junk food, that saturated fat only becomes a problem when combined with starch and sugar, and that instead of worrying about saturated fat itself, people should focus on their overall diet and personalised blood tests, which he promotes through his own company.
Let’s check if there is scientific evidence that supports this strategy.



The best available evidence still supports limiting saturated fat and prioritising unsaturated fats from nuts, seeds, plant oils, and other minimally processed foods to lower LDL‑cholesterol and heart disease risk. Hyman’s post selectively highlights real concerns about ultra‑processed foods while downplaying the role of saturated fat itself, skipping over the benefits of unsaturated fats, and steering readers toward expensive testing that does not replace basic, well‑supported dietary patterns.
Nutrition posts like this often look educational and science‑driven, but by cherry‑picking parts of the guidelines and skipping key context, they can nudge people toward eating more saturated fat than recommended and away from well‑established, low‑cost strategies like eating more plant‑based unsaturated fats. When the same message also funnels readers into a product the author profits from, the line between health education and marketing blurs, making it harder for the public to distinguish solid guidance from content designed to sell them something. Learning to spot these patterns is essential for protecting your heart health – and your wallet – in an information environment where confidence and visibility often overshadow balance and evidence.


The 2025–2030 US Dietary Guidelines on saturated fat: What changed and what didn't
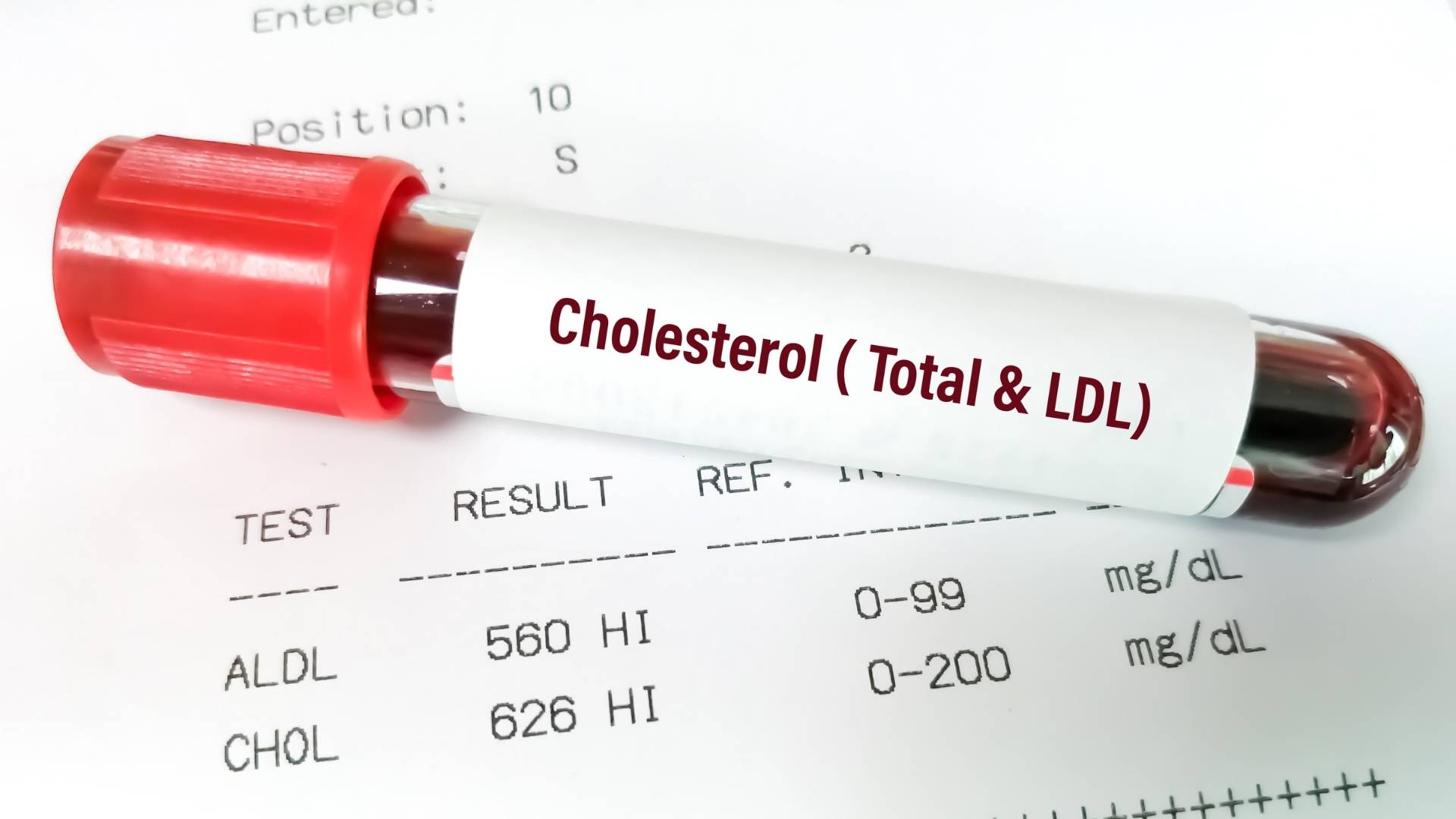
The 2025–2030 Dietary Guidelines for Americans (source) keep the long‑standing cap: saturated fat should not exceed about 10% of total daily calories. This limit remains because high saturated fat intake raises LDL‑cholesterol, which is a well‑established causal risk factor for cardiovascular disease such as heart disease or stroke (source).
To make sense of this, it helps to understand two common types of blood cholesterol:
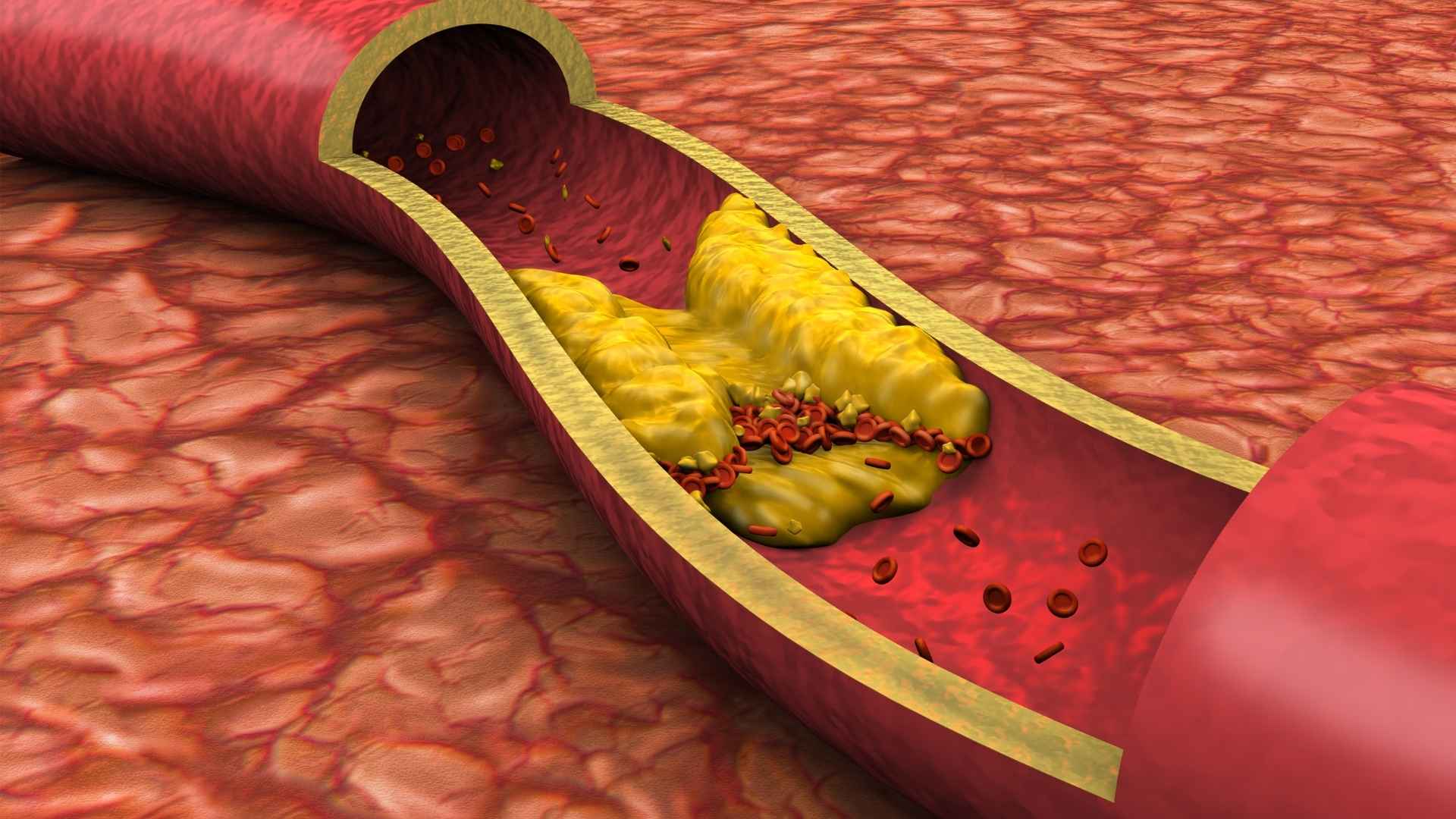
- LDL‑cholesterol is often called “bad” cholesterol because higher levels are linked to a greater buildup of fatty deposits in artery walls and a higher risk of heart disease and stroke.
- HDL‑cholesterol is often called “good” cholesterol because it helps carry cholesterol away from the arteries to the liver, where it can be processed and removed from the body.
Most major guidelines focus on LDL because, across many large studies, lowering LDL reduces the risk of heart attacks and other cardiovascular events, while changes in HDL are less consistently linked to outcomes. That is why the guidelines still set a clear upper limit on saturated fat: overall, eating more saturated fat tends to push LDL in the wrong direction, even if other parts of the diet matter too.
What is new – and can be confusing – is that the guidelines visually group foods like full‑fat dairy, butter, and beef fat directly under the heading of ‘healthy fats,’ while still stating that saturated fat should remain under 10% of total calories. This layout blurs the line between genuinely health‑promoting unsaturated fats and saturated‑fat‑rich foods, and several professional organisations (source, source) have pointed out that highlighting these saturated fat sources in a ‘healthy fats’ context sits uneasily alongside a numerical cap intended to limit them for cardiovascular risk reduction. For readers, it naturally raises questions: are saturated fats now considered ‘healthy fats,’ and if so, why are they still strictly limited?
Crucially, the guidelines and major expert reviews emphasise type of fat and replacement: reducing saturated fat and replacing it with unsaturated fats (good fats) is associated with lower LDL‑cholesterol and lower risk of coronary heart disease (source). Simply removing saturated fat and replacing it with refined starch and sugar does not improve – and can worsen – your lipid profile.
This is an important distinction: a creator can be technically correct that “context matters” while leaving out the main context public health bodies stress (the 10% limit and the benefits of unsaturated fats), which leads audiences toward a very different conclusion.
Claim 1: “Saturated fat from grass‑fed beef, eggs, and dairy is different from saturated fat in junk food”
Fact-check: The source of saturated fat matters mainly because of what comes with it, but at high intakes saturated fat from animal foods raises LDL‑cholesterol and heart disease risk regardless of whether it comes with a “healthy” or “junk” package (source).
Chemically, saturated fatty acids are the same molecules whether they are in a grass‑fed steak, a cheese‑topped ultra‑processed burger, or a pastry fried in beef tallow. What changes is the matrix: nutrients, fibre, sodium, refined starch, added sugars, and other fats bundled in the food. Whole foods like plain yogurt or unprocessed meat often contain protein, minerals, and little or no refined starch or sugar, whereas many ultra‑processed foods combine saturated fat with rapidly absorbed carbohydrates, low fibre, and high salt.

From a heart‑disease perspective, two questions matter: does the pattern raise LDL‑cholesterol, and what is the overall dietary pattern over time? Most ward studies and controlled trials show that replacing saturated fat with polyunsaturated fat (healthy fat) lowers LDL‑cholesterol, while replacing it with refined carbohydrate tends to have little benefit or can worsen LDL-cholesterol. This is where Hyman’s contrast – steak with broccoli and brown rice versus steak with fries and soda – has some truth: the second meal adds refined starch, sugar, extra fat from frying, and often trans‑fats, all of which can worsen cardiometabolic risk markers.
However, saying the “same saturated fat” is fine as long as the rest of the plate looks better jumps past the dose and the long‑term picture. Population‑level reviews (source) suggest that higher saturated fat intake tends to increase LDL‑cholesterol across diets, and that swapping saturated fat for polyunsaturated fat (healthy fat) is associated with fewer coronary events. Some analyses that look only at saturated fat in isolation and do not consider what replaces it find weaker associations, which is one reason headlines and influencers sometimes claim the “diet‑heart hypothesis is dead.” But when you focus on realistic substitutions – what people will actually eat instead – the pattern is clearer: moving from saturated to unsaturated fats appears beneficial (source).
The nuance around food matrices does not erase the underlying biology that saturated fat (particularly certain fatty acids) raises LDL‑cholesterol, especially when dietary cholesterol is also high.
Claim 2: “The real issue is saturated fat combined with starch and sugar – don’t replace saturated fat with carbs”
Fact-check: Combining saturated fat with refined starch and sugar is indeed a problem, but that does not mean saturated fat at high intakes is harmless; in a population that already eats more saturated fat than recommended, replacing some of it with unsaturated fat – not just any carbohydrate – improves LDL‑cholesterol and heart disease risk.
In the United States, most people are already over the recommended saturated fat limit before they ever add fries and soda to the plate. National survey data show that average saturated fat intake in U.S. adults is around 11–12% of total energy (about 28 g/day), with only about one‑third of adults meeting the less‑than‑10% target (source, source, source). Much of this saturated fat comes not only from desserts and fast food, but also from regularly eaten whole‑food animal products like unprocessed red meat, poultry, milk, cheese, and eggs. So when an influencer says the “real issue” is saturated fat combined with starch and sugar, it overlooks the reality that baseline saturated fat intake – including from whole foods – is already high for many people.

Several lines of evidence support the idea that replacing saturated fat with refined carbohydrates (like sugary food and drinks, baked goods, confectionery and foods made with white flour) does not reduce cardiovascular risk and can worsen lipid patterns, especially triglycerides (another unhealthy form of fat circulating in the blood) and LDL-cholesterol. Observational studies and controlled feeding trials show that when saturated fat is swapped for high‑glycaemic carbohydrates, LDL may fall modestly but triglycerides rise and HDL often falls, creating an atherogenic lipid profile overall (source). This is likely what Hyman is referring to when he warns against that particular swap, and on that narrow point he aligns with mainstream guidance.
However, the main alternative in modern guidelines is not “remove saturated fat and add white sugar,” but “reduce saturated fat and replace a meaningful portion with unsaturated fats and high‑fibre carbohydrates.” Meta‑analyses of prospective cohorts report that people who replace about 5% of energy from saturated fat with linoleic‑acid‑rich polyunsaturated fats (oils, nuts, seeds) have lower rates of coronary events and deaths (roughly 9–13% lower in some analyses) (source). Umbrella reviews (source) of randomized trials suggest that reducing saturated fat and increasing polyunsaturated fat (healthy fat) probably reduces cardiovascular events, although the exact magnitude depends on trial quality and context.
Dose and context matter. The LDL‑raising effect of saturated fat is more pronounced when dietary cholesterol is high, when overall saturated fat intake is substantially above recommendations, and when the diet is already rich in animal‑derived saturated fat. Weight loss, lower total carbohydrate intake, or shifts in LDL particle size can modify short‑term LDL responses in some individuals, which is one reason people can share very different personal lab stories. But none of this overturns the broader pattern that at population level – especially in a country where typical saturated fat intake is already above guideline levels – holding calories constant and moving from saturated fat to unsaturated fat is beneficial, particularly in people at elevated cardiovascular risk.
Framing the “real issue” as only the combination of saturated fat with starch and sugar can therefore be misleading. It draws attention to a genuine problem (ultra‑processed, high‑sugar, high‑fat meals) but downplays the fact that even saturated fat from everyday whole foods contributes to excess intake in many people, and that replacing some of this saturated fat with unsaturated fats and high‑fibre plant foods is one of the most consistently supported strategies for improving heart health.
Claim 3: “Precision nutrition and genetic differences mean saturated fat is only a problem for some – get a $365 blood profile”
Fact-check: People do vary in their lipid responses, but current evidence still supports general saturated fat limits and emphasises diet quality and unsaturated fats; genetic and lab‑based “precision nutrition” is not yet a substitute for basic healthy patterns and can be a vehicle for conflicts of interest.
There is real scientific interest in nutrigenomics – how genes influence nutrient responses. Some gene variants can affect LDL‑cholesterol response to dietary fat, and conditions like familial hypercholesterolemia (an inherited genetic disorder) make people especially sensitive to saturated fat and dietary cholesterol. But at present, large guideline‑setting bodies continue to recommend population‑wide saturated fat limits because the average effect is still LDL‑raising and because LDL‑cholesterol itself is causally linked to cardiovascular diseases like heart disease or stroke (source).

Routine cholesterol tests (total cholesterol, LDL, HDL, triglycerides) are useful, and using them to guide diet and medication decisions is standard practice in clinical care. However, the suggestion that everyone needs a subscription blood‑testing service to eat safely goes far beyond current evidence, especially when the same post omits simple, low‑cost strategies that are strongly supported by data: eating more vegetables, fruits, whole grains, nuts, seeds, and unsalted legumes, and using plant oils rich in unsaturated fat in place of some animal fats (source).
In this context, positioning “precision nutrition” blood testing as the natural next step after reframing saturated fat is problematic. The author promotes a specific, high‑priced testing service from a company that he co‑founded. While his Instagram bio mentions “Co‑Founder @function,” this connection is not clearly spelled out in the post where the service is recommended, and there is no obvious conflict‑of‑interest explanation for readers who may not click through his profile. Best‑practice guidelines for influencer marketing and health communication emphasise clear, upfront disclosures in or alongside promotional content; relying on a small profile tag that many viewers will never see seems to fall short of that standard.
For people trying to reduce their heart disease risk, standard lipid testing through usual healthcare channels, combined with established dietary patterns (more minimally processed plant foods and unsaturated fats, less saturated fat and ultra‑processed food), already has strong evidence behind it. By contrast, broad “precision” panels sold directly to consumers are still an emerging area with limited proof that they improve long‑term outcomes beyond what can be achieved with simpler, lower‑cost approaches. Framing these tests as the key to understanding whether saturated fat is “really” a problem for you can distract from well‑supported basics and, in this case, blurs the line between education and marketing.
Claim 4: “The guidelines now encourage plenty of animal protein and full‑fat dairy as part of healthy eating patterns”
Fact-check: The scientific consensus has not flipped to say that “plenty” of saturated‑fat‑rich animal foods and full‑fat dairy are risk‑free; current evidence still supports keeping saturated fat to about 10% of calories and centring healthy patterns that prioritise plant foods and unsaturated fats, with modest amounts of animal products.

The new guidelines’ wording and graphics give the impression that animal foods, including full‑fat dairy, steak, butter, and even beef tallow, sit right under the banner of “healthy fats.” Visually, steak, cheese, whole milk, and butter are given a prominent place in the new pyramid‑style graphic, even though the text still repeats the same upper limit of 10% of calories from saturated fat as previous editions (source). Several nutrition and cardiology groups have highlighted this as confusing, because it can easily leave people thinking the consensus has shifted to treating saturated‑fat‑rich animal foods as “healthy fats” in the same sense as olive oil, nuts, and seeds.
When we step back and look at well‑studied healthy patterns, the picture is different from “plenty” of animal fat. Traditional Mediterranean‑style diets, which consistently show lower cardiovascular risk, are not low‑fat overall but derive most of their fat from unsaturated‑fat‑rich plant foods (especially olive oil and nuts), with high intakes of vegetables, fruits, legumes, and whole grains, moderate fish and poultry, and relatively low amounts of red meat and dairy. In other words, these diets include animal protein, but animal foods are not unlimited, and saturated fat remains a smaller share of total energy than in typical Western diets.
Dairy is a good example of how nuance becomes social‑media confusion. Large cohort meta‑analyses generally find neutral or modestly protective associations between total dairy and cardiovascular outcomes, with some evidence that low‑fat dairy and fermented products (like yogurt and cheese) may be beneficial, while high‑fat milk can be neutral or slightly adverse in some analyses (source). Short‑term trials (source, source) often find that both low‑fat and high‑fat dairy can be relatively neutral for LDL‑cholesterol in the context of a controlled diet, but that does not mean unlimited full‑fat dairy is advisable in a real‑world diet where saturated fat is already above recommendations. The core message from major guidelines and reviews remains: dairy can fit into a healthy pattern, but total saturated fat from all sources should stay around or below 10% of calories, and unsweetened, lower‑fat or fermented options are often preferred when you look at the whole pattern.

Hyman’s emphasis on “plenty of protein from animal foods” and full‑fat dairy, without clearly mentioning the 10% saturated fat cap or the central role of unsaturated fats and plant foods, subtly shifts the takeaway from “these foods can fit in moderation” to “these foods are now the healthy core.” For readers, this can sound like the consensus has changed in favour of high‑saturated‑fat animal products, when in reality the underlying evidence and formal limit on saturated fat have not changed – what has changed is mainly the way the pyramid and “healthy fats” language visually highlight animal‑based options.
Saturated fat, unsaturated fat, and heart disease: what the research shows
To make sense of mixed messaging, it helps to separate three questions: what saturated fat does to LDL‑cholesterol, what happens when you replace it with different things, and what dietary patterns look like in real life.
On LDL‑cholesterol, controlled feeding studies (source) consistently find that increasing saturated fat (especially certain chain lengths common in dairy fat and meat) raises LDL‑cholesterol compared with unsaturated fats, with the effect size depending on baseline diet and cholesterol intake. There is individual variation, and other lipid fractions can change too – for example, triglycerides (a type of blood fat linked to heart disease) or HDL‑cholesterol (‘good’ cholesterol) may go up or down – but LDL remains the primary causal factor for cardiovascular disease like heart disease and stroke.
On replacement, large cohort studies and meta‑analyses (source) indicate that replacing part of energy from saturated fat with polyunsaturated fat (healthy fat) is associated with lower rates of coronary heart disease events and deaths. Replacing saturated fat with monounsaturated fat (e.g., from olive oil, avocados, some nuts) also appears beneficial, though effects can depend on the food source. In contrast, replacing saturated fat with refined carbohydrates and added sugars does not confer the same benefits and may worsen some risk markers (source).

On real‑world patterns, diets rich in minimally processed plant foods, whole grains, nuts, seeds, and legumes, with unsaturated fats as the main added fats and modest amounts of animal foods, are associated with lower risk of cardiovascular disease, type 2 diabetes, and obesity compared with patterns high in red and processed meat, refined grains, sugary drinks, and ultra‑processed snacks (source, source). Unsaturated fats, particularly from nuts, seeds, and certain oils, tend to lower LDL‑cholesterol or improve overall lipid profiles within these patterns (source).
This context makes it clear why major guidelines (source, source) still put an upper limit on saturated fat and encourage unsaturated fat‑rich foods, even while acknowledging that some whole‑food sources of saturated fat can fit in moderation. It also underlines what Hyman’s post leaves out: you do not need subscription blood panels to apply this evidence, and reducing saturated fat while increasing unsaturated fats from plant foods is one of the most consistently supported strategies in the literature (source).
Media literacy and food science: How to evaluate nutrition claims online
When you encounter nutrition content framed as “the truth isn’t what you think,” a few practical questions can help you evaluate it.

First, ask what is being compared. Hyman contrasts steak plus fries plus soda with steak plus broccoli plus brown rice, which correctly highlights the harms of ultra‑processed, starch‑and‑sugar‑heavy meals, but he does not contrast saturated fat with unsaturated fat‑rich alternatives like nuts, seeds, or plant oils, even though those swaps are central in expert reviews. A balanced piece would show multiple relevant comparisons, not just the one that flatters the preferred food.
Second, look for what official guidance actually says. In this case, the guidelines still cap saturated fat at 10% of calories and stress the benefits of unsaturated fats, but the post mentions neither, instead implying a broader “rehabilitation” of saturated fat. Visibility on social media does not guarantee that a summary faithfully reflects the source document.
Third, follow the money. When a post concludes that the real solution is a paid service or product – here, yearly blood profiling from a company the author helped found – that is a textbook conflict of interest that should be clearly disclosed. Undisclosed financial ties do not automatically invalidate every claim, but they should make you scrutinise the selectivity of the evidence and the omission of low‑cost, non‑commercial alternatives.
Fourth, notice how certainty is expressed. Strong claims that “we’ve been told X for decades but the truth is Y” often gloss over the fact that expert guidance has evolved by integrating new evidence, not by flipping 180 degrees. In the case of saturated fat, the main evolution has been toward focusing on overall patterns and replacements, not declaring saturated fat harmless.
Bottom line
Hyman is right that ultra‑processed foods combining saturated fat with refined starch and sugar are a major problem, and that whole, minimally processed foods are a better foundation. But by ignoring the 10% saturated fat cap, omitting the strong evidence on replacing saturated fat with unsaturated fats from plant foods, and tying the message to a commercial blood‑testing service he co‑founded, his post offers a partial and distorted picture of the science.
For the public, the most evidence‑based and accessible steps do not require precision lab profiles: keep saturated fat within recommended limits, avoid replacing it with refined starch and sugar, and prioritise unsaturated fats and minimally processed plant foods as the default, while recognising that individual preferences and medical conditions still matter and can usually be managed with routine clinical follow‑up and standard blood tests rather than intensive consumer subscription testing. Misinformation in nutrition often starts with a grain of truth – like the harms of ultra‑processed foods – but then narrows the lens in ways that align more with branding than with the full body of evidence; a useful rule of thumb is to ask whether a nutrition claim lines up with long‑term evidence and guidelines, or mainly with a brand’s business model.
We have contacted Dr Hyman and are awaiting a response.
Disclaimer
This fact-check is intended to provide information based on available scientific evidence. It should not be considered as medical advice. For personalised health guidance, consult with a qualified healthcare professional.
Stand Against Nutrition Misinformation
Misinformation is a growing threat to our health and planet. At foodfacts.org, we're dedicated to exposing the truth behind misleading food narratives. But we can't do it without your support.
Sources
- U.S. Dietary Guidelines. Dietary Guidelines for Americans, 2025–2030 (PDF).
- Hooper, L. (2015). “Reduction in saturated fat intake for cardiovascular disease.”
- Academy of Nutrition and Dietetics statement on 2025–2030 DGA release.
- American College of Cardiology commentary on 2025–2030 Dietary Guidelines.
- Center for Science in the Public Interest. “New Dietary Guidelines undercut science and sow confusion.” https://www.cspi.org/statement/new-dietary-guidelines-undercut-science-and-sow-confusion
- Li, Y. (2015). “Saturated Fats Compared With Unsaturated Fats and Sources of Carbohydrates in Relation to Risk of Coronary Heart Disease: A Prospective Cohort Study.”
- Siri-Tarino, P.W. (2010). “Saturated Fatty Acids and Risk of Coronary Heart Disease: Modulation by Replacement Nutrients.”
- Siri-Tarino, P.W. (2010). “Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease.”
- Lichtenstein, A.H. (1998). “Dietary Fat Consumption and Health.”
- Taylor, C.A. (2024). “Identifying the Leading Sources of Saturated Fat and Added Sugar in U.S. Adults.”
- Wambogo, E.A. (2023). “Dairy, Meat, Seafood, and Plant Sources of Saturated Fat: United States, Ages Two Years and Over, 2017–2020.”
- Farvid, M.S. (2014). “Dietary Linoleic Acid and Risk of Coronary Heart Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies.”
- Aramburu, A. (2024). “Effect of reducing saturated fat intake on cardiovascular disease in adults: an umbrella review.”
- Johnson, S.A. (2023). “Saturated Fat Intake and the Prevention and Management of Cardiovascular Disease in Adults: An Academy of Nutrition and Dietetics Evidence-Based Nutrition Practice Guideline.”
- Billingsley, H.E. (2018). “Dietary Fats and Chronic Noncommunicable Diseases.”
- https://www.foodfacts.org/glossary/mediterranean-diet
- Zhuang, P. (2025). “A global analysis of dairy consumption and incident cardiovascular disease.”
- Guo, J. (2017). “Milk and dairy consumption and risk of cardiovascular diseases and all-cause mortality: dose–response meta-analysis of prospective cohort studies.”
- Lamarche, B. (2025). “Regular-fat and low-fat dairy foods and cardiovascular diseases: perspectives for future dietary recommendations.”
- Wali, J.A. (2020). “Cardio-Metabolic Effects of High-Fat Diets and Their Underlying Mechanisms—A Narrative Review.”
- Clifton, P.M. (2017). “A systematic review of the effect of dietary saturated and polyunsaturated fat on heart disease.”
- Kenneth, R. (2024). “The Effect of Diet on Cardiovascular Disease and Lipid and Lipoprotein Levels.”
- American Heart Association. Saturated Fat. (https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/saturated-fats)
- NHS. How to eat less saturated fat. (https://www.nhs.uk/live-well/eat-well/how-to-eat-a-balanced-diet/eat-less-saturated-fat)



foodfacts.org is an independent non-profit fact-checking platform dedicated to exposing misinformation in the food industry. We provide transparent, science-based insights on nutrition, health, and environmental impacts, empowering consumers to make informed choices for a healthier society and planet.








.svg)
